By Felipe on November 09th, 2016. Posted under: 2016
Today we are living in a country in which more than 59 million people voted for a man who ridicules women, belittles racial and ethnic minorities, and threatens long-standing partners across the world. That is shocking in so many ways.
I have spent the past 30 years working toward ensuring that people can have the families that they want to have. That sounds like such a simple mission, but it is fraught with challenges from those who believe that the rights of those who can become pregnant should be subjugated to the “rights” of those not yet born. We have been fighting a war in this country for a very long time now and there have been victories on both sides, but yesterday was a huge loss.
Despite this loss, we are not powerless. All of us who work for Medical Students for Choice and all our members and alumni can and will provide the care that those who celebrate their victory today will attempt to deny. Looking forward, here are a few thoughts to consider:
We may lose legal abortion in parts of the US over the next several years. Well-trained abortion providers will be needed more than ever to care for women suffering from unsafe abortion.
Doctors will continue to be powerful advocates for their patients and your voices will be more important than ever.
All the skills that medical students learn at MSFC workshops, such as manual vacuum aspiration, will be skills that you may need to save the lives of your patients.
The Medical Students for Choice community will be gathering together in Phoenix, Arizona on December 3rd and 4th. If you hadn’t planned to join us, please consider joining us now! Contact meetings@msfc.org for more information. With 205 chapters in 32 countries, with thousands of alumni in communities throughout the US, Canada, and beyond, MSFC’s work is more important today than it has ever been. I am thankful for your courage, your passion, and your commitment…NOW MORE THAN EVER!
Lois Backus Executive Director of Medical Students for Choice
By Felipe on October 19th, 2016. Posted under: 2016
By Lindsey and Cyra, M2 Student Leaders
While neither of us came into medical school dead-set on OB/GYN or a career providing reproductive healthcare, both of us took for granted that a woman’s right to choose was something that all physicians should respect, regardless of their personal beliefs. However, as first year medical students it didn’t take us long to realize that not everyone believed in creating a safe, non-judgmental space to talk to our patients about their reproductive options, let alone to think about advocating for comprehensive reproductive healthcare.
In an atmosphere where a noticeable portion of the student body and faculty members were openly anti-choice, it would have been easy to avoid confrontation and to allow this important part of our education to be neglected. We felt isolated and afraid to speak up when the conversation turned in this direction for fear of isolating peers and potential mentors.
2015 Conference on Family Planning
However, MSFC’s 2015 Conference on Family Planning helped us to find our feet as students advocating for our educational needs, future reproductive health care providers, and future political advocates. At the Conference, we found a strong, powerful group of peers with whom to discuss and learn, and to gain confidence in making ourselves heard. We were impressed that the conference presentation did not shy away from controversial topics, but instead encouraged us to think like future clinicians who weigh scientific evidence and moral questions. The clinical sessions we attended helped fill in notable gaps in our education, provided us with hands-on skills, and taught us how to thoughtfully counsel patients who are contemplating their options.
Since returning to campus, we have fostered an atmosphere of discussion and education around reproductive health, organizing educational events to supplement our curricula as the leaders of our school’s MSFC chapter. Since we began to speak up, we have found more and more of our peers are willing to stand with us. Each time we have an event, we are surprised by the new faces we see and amazed by the growing receptiveness. We are witnessing the beginnings of strong advocacy for change on our campus, and hopefully in clinical practice beyond.
This year, we are coming to the Conference on Family Planning with two interested first-year students (and two newly-involved second year students!) who we hope will learn and become leaders in our chapter next year to carry this momentum forward. We want them to experience the inspiration and leadership development that we felt after last year’s Conference. We’re also coming back ourselves for a second year because it was impossible to do and see everything we wanted the first time around. While last year we stuck mostly to clinical sessions, this time we’re looking forward to attending more advocacy sessions, seeking out more on LGBT health, and getting fired up to continue to advocate when we come home. We are also both so excited to potentially try the Abortion Training Institutes as we move into third year.
The best thing about the conference is the feeling of finally being with your people- a group of motivated, high achieving future medical professionals that share the same priorities: the right to high quality reproductive healthcare for all, regardless of race, gender, sexual orientation, or the ability to pay. The conference reminds us why we went to medical school in the first place, and sends us back to school ready to face whatever comes our way!
By Felipe on September 08th, 2016. Posted under: 2016
As a first year medical student, I let my doubts get in the way of my education. I was intrigued by the idea of abortion education, but I missed out on Medical Students for Choice’s 2014 Conference on Family Planning because I wasn’t confident enough to make the trip alone. I worried that I would be judged for going and that my safety might be compromised.
That changed after becoming president of my school’s MSFC chapter. I felt compelled to learn more about abortion and family planning. I didn’t want to just say that I supported a woman’s right to choose; I really wanted to understand the issues surrounding reproductive healthcare. Together with my fellow leader, Claire Meikle, we dove head first into the world of Medical Students for Choice.
The author and her co-student leader.
We began the year by attending the 2015 Conference on Family Planning in Philadelphia, PA, and it was such an amazing experience! From the moment we arrived, we were greeted with open arms and were already known by name from our previous MSFC leadership involvement. We heard from amazing speakers from all over the world (we even made our moms attend so we could attend *every*single* breakout session!). We connected with leaders of other chapters and learned some amazing content that we then brought back to improve our own chapter. At the conference, I was able to not only learn more about reproductive health care, but also gain a better understanding of my own beliefs. I was encouraged to push myself out of my comfort zone to continue my abortion education. I took all that I had learned from the conference and all of the questions that I still had and carried them with me to the Abortion Training Institute later that year. Since then, I developed an entire Family Planning course for our school and am currently leading a research project on family planning education for medical students.
No matter how far you are into your medical education, you will gain so much from MSFC’s conference! From the guest speakers to the hands-on training sessions, there is something for everyone. No matter your hesitation, fear not—the CoFP is a safe and welcoming place to start or expand your family planning education. (Plus, it’s a great excuse to travel!)
While I know that medical school can be overwhelming and there’s never enough free time, attending MSFC’s Conference on Family Planning in Phoenix, AZ on December 3rd and 4th is a valuable experience that is worth the time away from campus.
Are you convinced yet? Ready to register? Click the link below to sign up!
By Felipe on August 17th, 2016. Posted under: 2016
By Brooke Bachelor, RN, BSN, OMS-II
My interest in exploring and working within various health care systems has led me around the world. In each country I visit, I strive to understand the intricacies of each unique health care system, and more specifically, the cultural components of reproductive health care. Having worked with many patients from Mexico during my time as a nurse in the US, I knew an MSFC Reproductive Health Externship (RHE) in Mexico City at Clínica Acompañame de Centro de Atención Integral a la Pareja A.C. was a perfect match for me as a future physician exploring a career as a safe abortion provider, primarily for Spanish-speaking patients.
BACKGROUND:
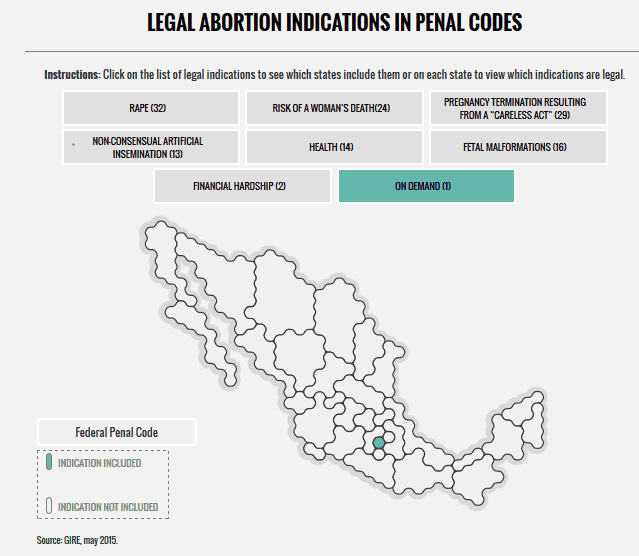
According to the Grupo de Información en Reproducción Elegida (GIRE), abortion in Mexico is regulated on a local level, with each state establishing its own rules regarding safe abortion access. Elective abortion through the first trimester has only been legal in Mexico since 2007, and even then, only in the Federal District of Mexico City. To put this in perspective, this means that the area where abortion is legal, safe, and elective only covers about 1% of the country, or as little as is depicted by the area shaded in blue on the map below.
Source: GIRE, May 2015
Unfortunately, this lack of access to safe and legal abortions directly translates to unsafe abortions being the fourth leading cause of maternal mortality. Mexico, like the US, is failing to provide an adequate amount of safe abortion services to meet the needs and demands of the country’s population.
In all Mexican states, an abortion for a pregnancy resulting from rape is technically legal, but in practice, women’s access to services are often limited. In states like Guanajuato, there are no regulated procedures in place to help a woman access a safe abortion. While learning this, I couldn’t help but think of the parallels between this system and the TRAP laws in the US, where abortion may be legal on paper but difficult to access for a variety of reasons.
As we’ve seen repeatedly in countries around the world, restrictions on abortion do not prevent their occurrence. More than one-third of women receiving a clandestine abortion are expected to have complications that require medical treatment. Of those women, an estimated 25% do not receive the hospital care they need.
EXPERIENCE:
Before the RHE, I firmly believed that safe, legal abortion should be available to women everywhere, but I was unsure of how I would react emotionally to seeing an abortion being performed for the first time. I can tell you that the first time I observed an abortion procedure, I said, “That’s it?” This realization of how simple and safe the procedure is, along with seeing the physician’s ability to change lives for the better in a short period of time, strengthened my desire to do this important work.
I was impressed by the clinic’s comprehensive and holistic approach to patient care. Each patient considering abortion had to go through the same screening steps each time to address their specific needs and to be medically and psychologically cleared for an abortion, whether through medication or surgical procedure.
After an initial consultation, women were counseled about how they came to their decision and were able talk openly about any doubts or reservations alone and/or with significant others and family. I quickly learned while hearing the stories of patients that these were not last-minute decisions women made. If a woman chose medication and the option was available to her given her situation, the process was explained to her. After asking any remaining questions, she took a few medications to start the abortion process and was provided an emergency phone number in the rare case that she needed to contact a doctor. If an women opted for the abortion procedure instead of medications, it usually only took about 15-20 minutes from start to finish, and after about 15 minutes in the recovery area, most women walked out of the clinic to continue their lives.
I was so impressed that the clinic not only provided abortions, but also focused much of its effort and energy on preventing these unwanted pregnancies in the first place with subsidized LARCs (long-acting reversible contraception) and other contraceptive methods. The clinic also offered general women’s health consultations and vasectomies.
LESSONS:
Having witnessed this massive gap between need and provision of safe abortion services in Mexico and all over the world, I feel especially motivated to pursue this career path. Here are a few major learning points and important reminders from my experience at Clínica Acompañame:
From a more practical and professional standpoint, I left my RHE well-equipped linguistically to work in reproductive health as a physician with Spanish-speaking patients. I learned a lot of Spanish vocabulary for specific medical terms that I didn’t even know yet in English.
Seeing the difference in patients’ outlooks on life before and after an abortion instilled in me the importance of medical schools exposing students to abortion care, even at a basic level. We have the responsibility as health care professionals, regardless of our personal views, to know what resources are available in our communities and, at a minimum, be informed enough to discuss all reproductive health options with women.
55% of pregnancies were unintended in Mexico in 2009, so this highlights the need to focus efforts and funding on the prevention of unwanted pregnancy through education and easy access to affordable LARCs.
It is imperative that BOTH parties each take responsibility for his or her reproductive potential for contraception to be effective. All too often, this responsibility unfairly falls solely upon the woman.
Even with the victories during the last decade for Mexican women that have led to increased safe abortion access, we can and should do more. We must work together as health care professionals and as a society to make sure abortion is accessible, which will undoubtedly save the lives of countless women. I look at the large gap worldwide between need and access to safe abortion services, and as a future physician, I find myself wondering…if not me, then who?
In June, I started my Reproductive Health Externship (RHE) at Houston Women’s Clinic in Houston, Texas. Houston Women’s Clinic (HWC) is a standalone abortion clinic (not an ambulatory surgical center) and is one of eleven clinics left in the state. When I was setting up my externship with Kathy, the clinic manager, we discussed the Whole Woman’s Health v. Hellerstedtcase. Kathy let me know that if Whole Women’s Health lost the case, the clinic would close. We planned for me to start on June 1st so that I could spend as much time as possible in the clinic before the Supreme Court made a ruling.
In those first few weeks, I spent time with the counselors, ultrasound technicians, nurses, and observing the doctor in the procedure rooms. Every single day, the clinic was operating at the peak of its capacity as women came from all over Texas and Louisiana to receive abortion care.
While the staff was clearly focused on serving our patients, there was an undercurrent of fear for the clinic’s future. They told me how they had to close for over a week until HB2 was suspended and how stressful it had been to have their jobs hanging in limbo. Everyone was worried that the clinic may have to shut down, and it was unclear if they would be able to move to a surgical center to keep providing abortion care. The staff aimed to hide these concerns from patients, but I remember when a patient needed to schedule her procedure for the third week of June, no one knew if the clinic would still be open then.
I took a hiatus from my externship at the end of June, but after the Supreme Court released its decision, Kathy invited me to come back for the rest of the summer. Since I’ve been back at HWC I have been talking to the staff about the SCOTUS decision and what it means to them. The day the decision came out, everyone was overjoyed and excited but there was no time to celebrate because of all the patients waiting for counseling and procedures. A celebratory cake was brought in for lunch, but nobody got a piece until after the last patient left that afternoon. The SCOTUS ruling was exciting because it reaffirmed abortion rights, but it also meant everyone at HWC could breathe easier knowing they would be keeping their jobs.
One aspect of the fight against TRAP laws and abortion restrictions I don’t see discussed very much is how they impact the nurses and staff who work at abortion clinics. The lack of job security that follows the litigation of TRAP laws puts incredible stress on clinic employees whose jobs are stressful enough already. It was deeply gratifying to see these incredible women who have taught me so much able to stop worrying about losing their jobs at a moment’s notice.
When I discussed the SCOTUS ruling with the staff, one woman told me how glad she was the HWC would continue to stay open, not just for her job’s sake, but because she viewed the clinic as an important part of the community. She told me about driving two of her friends to the clinic to get abortions when she was in high school. One of the nurses told me she was happy that the ruling finally showed an understanding that surgical regulations are medically unnecessary for abortion care and that she hoped more clinics will re-open, especially on the gulf coast of Texas and in Louisiana.
One woman who has worked at the clinic since the early 1980s was amazed at how few patients knew about the WWH v. Hellerstedt case at all! On June 27th, the day of the Whole Woman’s Health decision, the nurses and medical assistants in the procedure rooms applauded the doctor as he came in to perform the first abortions of the day. Afterwards, a medical assistant told me that patients asked her if they clapped every day, not knowing about the case at all.
Though we celebrated after work that day at a Planned Parenthood rally, since then it’s just been busy as usual at HWC. We still have nearly 100 patients a day coming in for counseling and procedures who make the trek from all over Texas and Louisiana to access safe, compassionate abortion care. I try to make a point of talking to patients about their rights and encouraging them to be more politically active. When someone comments about how crowded the clinic is, I make sure to tell them that back when Texas had 41 clinics, crowding wasn’t such a problem. Now that we are only one of 11, we have many more patients. Hopefully, thanks to the SCOTUS ruling, more clinics will open back up and women will be able to access abortion care closer to home. Until that happens, Houston Women’s Clinic’s doors will be wide open.
On Monday morning, the Supreme Court made the momentous decision to overturn Texas’s HB2 law. The highest court in the country decided that Texas’s TRAP laws placed an undue burden on women seeking an abortion. However, there is still work to be done in Texas and many other states. One of the biggest obstacles facing women and the abortion clinics that seek to serve them is a lack of abortion providers. This is not a new problem.
Twenty-three years ago, our founder Jody Steinauer was a medical student at University of California San Francisco. She, like thousands of other medical students, received a mailing which included the following “joke”:
Q: What would you do if you were in a room with Hitler, Mussolini, and an abortionist and you had a gun with two bullets?
A: Shoot the abortionist twice.
Sadly, this “joke” has become somewhat true and timeless. Since 1993, the year Medical Students for Choice was founded, eleven people have been murdered due to anti-choice violence. Three of those murders happened last year in Colorado Springs, CO. According to National Abortion Federation, besides the eleven murders previously mentioned, “Since 1977, there have been […] 26 attempted murders, 42 bombings, 185 arsons, and thousands of incidents of criminal activities directed at abortion providers.” From 2014 to 2015, death threats increased from one to 94. Given these grim statistics, coupled with the lack of education and training available to future abortion providers, it is no surprise that the number of abortion providers in the US has dropped drastically.
This is exactly why Jody started MSFC. She knew, as did abortion opponents, there is no choice without trained and willing providers. This is why medical students around the world have sought out MSFC for education materials, training, and funding for externships. This is why medical students have founded their own chapters on their medical school campuses across the US and around the world. This is why MSFC stands up in the face of opposition.
Medical Students for Choice fights not just for the right to an abortion from a trained medical provider, but also the rights of medical students who want a comprehensive education on reproductive health care. We exist not just for the women with unintended pregnancies, but also for the doctors who counsel them. We work every day for women who want an abortion for whatever reason they choose, and for the providers who will keep them safe. Without providers, there is no choice. Without education, there will be no providers.
The author and her chapter co-founder at graduation.
By Christina Bourne
Being pro-choice has always been natural to me. I grew up in a pro-choice family, had an abortion as a teenager, and never felt anything but support from my community. I seldom thought about the right to choose. Sure, I knew there was debate around the issue, but I never felt a strong need to engage. I just assumed that we lived in a country where the right to have an abortion was and would continue to be a reality.
My assumption was challenged in 2012 when I started medical school in Wichita, Kansas, and it became clear to me that not everyone was pro-choice. I quickly bonded with a fellow medical student, Claire Thomas (on the right). The two of us often felt like progressive spirits swimming upstream in a sea of conservatism. We had each other, and sought to build community around issues we were passionate about.
When Claire and I realized that our campus didn’t have a chapter of Medical Students for Choice, we made it our mission to start one. But it wasn’t as easy as we had hoped. At the time, Wichita physicians still felt the aftermath of the 2009 murder of Dr. George Tiller – a local abortion provider and community leader. It took us two whole years of asking before we finally found a willing faculty advisor for our MSFC chapter – a requirement to form any student group.
Claire and I were so excited to have our “official” group on the books…only we had no idea where to start. During my spring break, I called the MSFC headquarters, hoping to get some direction. It was such a breath of fresh air. I talked with the Manager of Student Organizing for over an hour about the anti-choice state I lived in (Kansas), how long it had taken us to get a chapter started (two years), and what training we had received about abortion care and management (little to none). Besides my conversations with Claire, I truly felt heard and understood for the first time.
Facing adversity was not new for MSFC headquarters staff, and they knew exactly how to help get my chapter up and off the ground. I smile as I look back on that phone call because it was the moment that ignited our group. At the end of the call, I already had resources in my inbox, a welcome packet sent to my home address, and a plan for our first school meeting.
Since that day, our group has been one of the most active student organizations on campus. To date, we have held lectures on birth control, an MVA training workshop, an IUD training workshop, a vasectomy lecture, an ethics discussion, planned and hosted a transgender healthcare panel, participated in community canvassing, and helped plan a women’s health fair. We have partnered with Wichita’s Planned Parenthood and our local women’s health clinic which provides full spectrum healthcare. We printed and sold MSFC shirts and had an e-fundraiser to send two of our chapter members to MSFC’s annual conference. And last year, Claire and I attended MSFC’s Abortion Training Institute where we were able to unload, connect and network with our peers and current abortion providers.
The main reason our chapter has been so active is because of the awesome staff at MSFC. They understand the hectic schedules of medical students and provide power points, educational handouts, video tutorials and all the supplies needed to host educational events. Staff are extremely easy to get ahold of and quickly answer any questions that allow us to effortlessly put together these events. Words cannot express how deeply supported we have felt these past two years.
Without our MSFC chapter, abortion would rarely be discussed on the KU-Wichita medical campus. It has simply not been a part of our curriculum. Moreover, a year ago, a new chapter of Medical Students for Life was created on our campus. I like to think that this would not have happened if our chapter of MSFC was not as active.
Our MSFC chapter has brought a vital forum for balanced discussion on issues surrounding women’s health to our campus. Just last month we held an event which covered birth control and medical abortion, and we discussed current legislative restrictions and TRAP laws. First year medical students expressed surprise – they said they hadn’t been aware of the extent of Kansas’s restrictive policies towards women’s health. Later, they personally thanked us for generating this discussion. We also got a few new members.
I want to give a giant shout out to everyone at MSFC and specifically to the providers I have worked with along the way that have helped me build my medical and ethical foundation. I continue to feel supported and embraced by my MSFC family, and MSFC is the reason that I am going to be a provider. I am about to start my residency in Family Medicine and Psychiatry at UC Davis, where abortion training is integral to the curriculum and spirit of the program. Claire, meanwhile, will be moving to Fort Worth, TX to keep fighting the good fight as a Family Medicine Resident and future abortion provider at John Peter Smith Hospital. Our bond continues to grow, strengthened by our experience as MSFC co-presidents. We can’t wait to continue working with MSFC as MDs, during residency and beyond!
Yesterday, lawyers for the ACLU and the Center for Reproductive Rights embarked on oral arguments before the Supreme Court for what is being called the most important abortion rights case in decades. In 2013, the Texas House of Representatives passed House Bill 2 which, among many other new restrictive regulations, requires abortion providers to hold admitting privileges at nearby hospitals and imposes ambulatory surgical center requirements for all clinics where abortions are performed. Now, in Whole Woman’s Health v. Hellerstedt the Supreme Court will decide whether HB2 places an undue burden on a woman’s right to terminate a pregnancy. For the women of Texas, the impact of HB2 is clear: women will travel farther to find a clinic and incur higher costs, longer wait periods, and more invasive procedures with no increase in the safety of the procedure. For the record, an abortion performed by a skilled physician has a 0.05%-0.2% risk of major complications.
What remains less clear, and certainly less talked about, is the impact HB2 will have on the medical students in Texas. Training and education in abortion care is already difficult to obtain for medical students, particularly in the Lone Star State.
Across the US we know that two-thirds of medical schools spend less than 30 minutes of class time on all aspects of abortion throughout the four year medical education. This means that for future doctors who want (and need) to be prepared to meet the reproductive needs of their patients they must seek training outside of their medical program. Most often this comes in the form of receiving training at a local clinic. What will this look like in Texas if HB2 is allowed to go into effect? It’s impossible to know with any certainty, but if current numbers are any indication, training in Texas could grind to a virtual halt.
Each year Texas graduates roughly 1,700 medical students, and 58% of those graduates remain in Texas for residency. With only 10 clinics providing abortions, and each abortion provider needing to retain admitting privileges with a nearby hospital, even if only a fraction of medical students or residents seek out training, the feasibility of training to competence becomes nearly impossible. And without opportunities for future physicians to learn, Texas could easily become a state without any abortion care in a few short years.
A Supreme Court decision which does not explicitly strike down HB2 not only harms today’s women, but places future generations of women at risk as well.
HB2, previously upheld by the 5th Circuit Court of Appeals, will go into effect in the event of a 5-3 decision in favor of Hellerstedt or in the event of a 4-4 decision with the current even number of justices. For the sake of women everywhere and the medical students, residents, and physicians dedicated to providing abortion care, we hope medical knowledge and not political grandstanding prevail in the coming months. However, regardless of the outcome, Medical Students for Choice will remain steadfast in our mission to create tomorrow’s abortion providers and pro-choice physicians. Today, more than ever, it is important for us all to remember that without providers, there is no choice.
Abortion restriction laws have sadly become the norm in many states in the U.S. Though many of these laws are passed under the guise of helping women, they are actually made with the intent to slowly legislate abortion until it is virtually inaccessible. One tactic we are seeing in increasing numbers is the institution of waiting periods. Last summer, the Florida House of Representatives passed such a bill. HB 633 requires any woman seeking an abortion to wait 24 hours between her initial consultation and the actual abortion procedure. Though the bill was initially signed into law, a state judge issued an injunction blocking the new law from going to effect.
MSFC is a co-plaintiff in the case against this law, and we stand alongside The Center for Reproductive Rights, the American Civil Liberties Union, the ACLU of Florida, and Bread and Roses Women’s Health Center in the effort to overturn this legislation. On February 9, 2016, several of our student activists, including Jessica Brosch and Katherine Somodi-Stephenson, were present in court to hear the beginning of arguments around the new law.
As plaintiffs in this case, our main argument against HB 633 is that it violates a Florida woman’s right to privacy. The Florida Constitution states that “[e]very natural person has the right to be let alone and free from governmental intrusion into the person’s private life.” HB 633 is an intrusion by the government into a woman’s reproductive health care choices and implies that Florida legislators believe women are incapable of making their own decisions regarding their bodies. As Katherine pointed out, lawmakers “claim time and time again that the law is somehow empowering to women. If women had to wait 24 hours after their driver’s test to get their license, to really think about if they wanted to deal with the danger of driving and its effects on their lady-brain…no one would call that empowering.”
Perhaps equally important is that this bill would present women with logistical obstacles they may not be able to overcome or afford, and may be especially difficult for low-income women, victims of rape or incest, and women whose fetus has a fatal anomaly. Jessica illustrated how this would impact women who seek care at her university’s clinic: “our local [University of Miami] hospital clinic only performs procedures on certain days of the week, so a 24 hour waiting period could easily turn into a 4 or 5 day delay depending on availability of clinic appointments. Scheduling each patient for two appointments also cuts into the time available to see other patients, who are often visiting for routine gynecologic care and contraception counseling, the very types of appointments that, if more readily accessible, could help reduce the need for abortions.” Further, Jessica pushes us to imagine a working mother having to deal with the 24 hour requirement. “Transportation to clinics, finding childcare or taking time off of work or school will turn a simple process into a cumbersome hassle at best, and at worst blocks access to care while demonstrating the State of Florida’s mistrust of women.”
For now abortion access remains threatened in Florida. And we, along with our many allies, are working hard, both inside and outside of the courtroom to change that. In an ideal world, political ideology would not affect judicial decisions. We hope the judges will come to the conclusion that women who seek abortions have just as much of a right to privacy as everyone else in Florida. But as Katherine put it, “maybe [we’re] biased.”
By Tiffany Stainfield, MSFC Chapter President at Ohio University Heritage College of Medicine
After four consecutive near-sleepless nights, tons of research into economic and social implications for Ohio, hours of proofreading and editing testimony, and two hours driving to Columbus, I spoke to the Ohio Senate on January 27, 2016 in opposition to House Bill 294. Instead of studying for school like every other medical student in my class, I wrote the most compelling testimony I could personally imagine in support of Planned Parenthood Ohio – only to be rejected by a group of conservative, lobby-minded, religiously-fueled Ohio Senators, who already knew how they were going to vote when they walked onto the Senate floor that morning. After a whole 15 minutes, a group of old white guys decided that they were going to defund Planned Parenthood.
Okay – that may not exactly reflect the Senate Committee meeting that morning, but it’s what it felt like. It is heartbreaking as an Ohio woman, MSFC chapter founder, future physician, and abortion recipient to stand in a room and urge a group made up entirely of men to allow Planned Parenthood to stay open in Ohio. I know there is no federal or Ohio state monies used to fund abortion services. I know it is the STI testing, cancer screenings, low-cost contraception, and prenatal care that will be taken away from over 155,000 women in Ohio that go to Planned Parenthood annually. And I know as I watch as the passage of HB 249 cut $1.3 million from any “entity” that provides elective abortion, Planned Parenthood is the obvious target.
I based my testimony on the following argument: If the goal is to reduce the overall need for elective abortion in Ohio, how is it possibly the answer to take away the very means that prevents unwanted pregnancies in the first place? I tried to appeal to their fiscally-minded nature, arguing that by defunding these “entities” and Planned Parenthood in particular, the overall healthcare costs in Ohio will rise, with increased cancer, STI, and pre-term birth treatments needed, and more unwanted births occurring. Unfortunately, the now-viral LA Times article about the increased number of “poor” Texas births occurring after the defunding of abortion clinics in Texas had not yet been released, though I gladly sent Ohio Governor Kasich the article to further support my testimony.
Though we may have been unsuccessful that day, I fully realize that it is in my voice, my power as a future physician, and my unrelenting pressure on the legislators of this state that will make a difference. And it is combining my voice and power with others’ on our side that will truly change the course of history. MSFC chapters across Ohio have been working together in letter writing campaigns, testifying at the Statehouse, and even forming petitions for Governor Kasich to veto HB 294. Though we all realize PP Ohio is about to lose $1.3 million any day now, eventually being forced to close the doors of the few clinics left, it is incredibly inspiring to realize that future abortion providers are coming, our voices will be heard, and we will not back down. This story will continue.