By Felipe on November 02nd, 2018. Posted under: 2018
Under a siege of anti-choice rhetoric at the national level, New York has felt like a ‘safe place.’ Abortion was legalized here in 1970 before Roe V. Wade, a provider assured me during my medical school interview. Hearing this, and knowing of New York’s historically blue political leanings, led me to idealize the state of abortion access in New York. I would soon be surprised at how much resistance there is here towards simply keeping abortion legal.
Medical school was an opportunity to connect medicine to public health and policy, and to learn how to marry my professional career with my activism. Throughout college, I supported the fights for health access, labor rights, and climate change. I helped organize rallies for divesting our university endowment from fossil fuels and for passing single-payer insurance at the Massachusetts statehouse. I joined the Massachusetts organizing team for the 2017 Women’s March in DC, which brought thousands of Massachusetts residents to the capital. I see these social issues as key to ensuring a healthy environment and access to healthcare for all.
But in my first year of medical school, I did not find any opportunities to learn about how providers do political advocacy. An email from Physicians for Reproductive Health (PRH) alerted me to the Reproductive Health Act (RHA), an update to New York State’s abortion law of 1970. As I read more on the RHA, I began to realize that New York’s laws were not as progressive as I thought. For example, the penal code still includes performing an abortion as a crime. Of course, this is not enforced because Roe V. Wade is a federal decision. But with Roe facing threats, passing the RHA and protecting abortion access in New York is imperative.

The author (L) and her classmates Katie DeWilde and Amanda Orley.
PRH organized a lobby day for providers to testify to their state reps on the Reproductive Health Act. I was frightened by the prospect of Roe being overturned, but emboldened by my desire to see physician-led advocacy first hand. Our MSFC chapter went to work. In preparation, we hosted a letter-writing session where we testified in writing to our state senator and the chairman of the health committee. Three of us then drove to Albany to speak to our representatives in person alongside the rest of the PRH cohort. On the ride up, I felt the weight of the hand-written letters in my bag and the light-headedness of excitement. When we spoke with our representatives, I was nervous and felt my face flushing, yet the more I spoke, the more confident I became. I heard confidence in the voices of my classmates, too, and I felt proud to be testifying alongside such passionate and determined future-physicians.
However, the RHA and the Comprehensive Contraception Coverage Act (a bill that would protect access to contraception) did not even make it past committee. In fact, the Reproductive Health Act has been introduced in committee every session for years but has never passed. We urged our state senator, a co-sponsor of the RHA and CCCA, to be a stronger advocate for these bills, even while knowing that he has a record of voting along with his Republican colleagues. We knew it was an up-hill battle as current state senators in New York have never had to vote on an abortion bill before. While they may have campaigned in support of women’s rights, voting on the record has proven too politically risky.
If Roe gets overturned, a woman in New York could go to jail for attempting a self-induced abortion. An abortion provider could be charged with a felony. We cannot stand by as medical students and assume our opinions don’t matter because we’re young, because we’re not yet ‘experts’, or because we’re in a ‘blue state.’ Testifying makes a difference. It shows our representatives that the stakes of these bills are real, and that it is not just their political reputation on the line, it’s human lives.
Editor’s note: if you live in New York, you can find your state senator’s position on the Reproductive Health Act at www.choicechamps.com. MSFC does not endorse or oppose candidates.
By Felipe on October 10th, 2018. Posted under: 2018, News and Views
On Saturday, the US Supreme Court gained a clear majority of members prepared to overturn nearly 50 years of legal abortion in the US. No matter how you may feel about the new Justice himself, the balance of the Court will negatively affect reproductive justice for years to come. The impacts of future Supreme Court decisions will be broad, and one of those impacts will be fewer doctors able to perform abortions.
Our colleagues at the Center for Reproductive Rights predict that 22 states will lose legal abortion if Roe v. Wade is overturned or gutted. Unfortunately, 80 medical schools are in those 22 states. So what will it mean when all the doctors graduating from all those medical schools have no medical knowledge or skills related to abortion?
Unless we start working now to nurture medical professionals trained and willing to provide safe abortions, regardless of whether abortion is legal in their states, the loss of a qualified medical workforce will greatly worsen the loss of legal abortion for those who seek it. It will also exacerbate the consequences for those that, in desperation, seek unsafe abortions.
Prior to the Court’s legalizing abortion in 1973, some doctors provided safe abortions to patients despite the possible legal consequences because they were compelled by their conscience and compassion for those they served. The unfortunate experiences they had caring for hundreds of thousands of women in hospitals suffering from unsafe abortions gave them the skills they needed to safely provide this care. Today, the loss of education and training that would result from overturning Roe would leave large areas of the US, within just a few years, with few doctors trained to provide…and those doctors will be aging.
I was in high school when the Court legalized abortion in the US. The Roe decision didn’t just pop up out of nowhere. It came after years of dedicated effort to change the way abortion was viewed by the American public, an effort that led to the liberalization of abortion laws in 17 states prior to the Court’s decision. Today, we are facing another long period of effort focused on preventing access to abortion from sliding back too far and then pushing the pendulum back toward a saner, safer view of abortion access.
Physicians, and all medical professionals, will be critical to that effort because they will be on the front lines in the fight to maintain access to safe abortion, and where that is no longer possible, to save the lives of those suffering from unsafe abortion. Medical Students for Choice is at the center of the effort to ensure that medical students have an opportunity to gain the skills and knowledge, and to nurture the courage needed to facilitate care for the most vulnerable.
MSFC is uniquely positioned to do this with chapters at 158 medical schools in the US. MSFC members are active in every region and almost every state including Alaska and Hawaii. More than half (85) of MSFC’s US chapters are in politically conservative states. These are states, such as Texas and South Dakota, with legislatures determined to limit access to abortion and eager to eliminate access to abortion entirely if Roe’s protections are taken away. Having directly experienced the many impacts on access coming out of their states’ legislatures over these past years, our members are well aware that Roe’s protections cannot be taken for granted. Helping their patients get to clinics that may be hundreds of miles away has become commonplace for many of our members in these states.
Abortion knowledge and skills are essential for doctors because they are the same skills they will need to help those suffering from unsafe abortion. The devastating injuries and deaths resulting from unsafe abortion happen everywhere, worldwide, in places without access to safe, legal abortion. Without physicians with the knowledge or skills in abortion, women will unnecessarily die or suffer long-term injuries. That’s a fact.
MSFC is not sitting by and waiting to respond to those horrifying outcomes. We are preparing every chapter in those 22 states to fill the educational needs for their fellow students and supporting our chapters’ involvement in both institutional and state-wide advocacy campaigns. We have a plan and we have already begun to implement it.
As difficult as these times are for all of us who care so deeply about equity and social justice, working with young people who are passionate about these issues is a real privilege. I know that thousands of MSFC members will help push the pendulum of change back toward care and compassion. And although many MSFC chapters will be directly affected by any US Supreme Court changes to legal abortion, many are also in states where abortion is expected to remain legal. As a community, we will pull together to ensure that interested students from poor access states will be able to seek education and training elsewhere. Our hundreds of abortion-providing alumni are already stepping up to support students in states like Arizona that prohibit abortion education in their state schools.
Hope, persistence, and a vision of what we want our world to be like will carry us through these challenging times. We can only hope that reason will prevail in our courts and legislatures, but with a relatively young majority on the Court that opposes the Roe decision, we have many years of hard work ahead of us. MSFC already has changed, fundamentally, the way that the medical profession views abortion and family planning. As we move forward from here, I know that regressive values cannot stand long against the hundreds of MSFC members graduating from medical schools each year.
By Felipe on September 19th, 2018. Posted under: 2018

Coming from a background in sociology and anthropology, I chose medicine as a career because I believe that health is foundational to all other social justice work. I am pursuing a combined MD/MPH because I aim to put my clinical practice in a broader context—to better understand the systems within which medicine operates. The system is flawed and continues to deny the basic human right of health to those who need it most. The right to control what happens to one’s own body is, in my opinion, one of the most basic human rights, and I cannot think of a more honorable way to spend my life than by helping women feel in control of their bodies, and hopefully also to play a role in helping women feel empowered in their bodies.
That is why I decided to participate in MSFC’s Reproductive Health Externship after my first year of medical school. I knew this experience would allow me to further my commitment to reproductive justice by providing me the opportunity to start actually seeing procedures, an important step towards gaining the concrete skills necessary to provide abortions and to do the work that I so deeply believe in.
During my RHE, I spent the first part of this summer at a family health clinic in the Bronx learning about reproductive justice and abortion under the supervision of some of the most inspiring and bad-ass women I have ever met. More than any other time in my life, I feel like I know what I want to be when I grow up: I want to be just like them—doctors who listen, who inform, who support, who care, and who treat individuals with respect, with compassion, and with dignity.
In a lot of ways I feel like medicine has been this thing that I’m doing, that’s still somewhat separate from the rest of my identity. And then on my first day in the Bronx, I ended up in a room full of residents having a conversation about the many messages that women receive from different parts of our lives telling us that our bodies are wrong, and talking openly about the ways that doctors both contribute to and can combat against this and help normalize the female body. I saw a presentation by residents working to change systems to be more gender inclusive. I attended a lecture about birth justice and the enormous racial disparity in maternal mortality that exists in this country and especially in NYC. Being surrounded by doctors who are similarly committed to social justice was a real game changer for me, and I honestly didn’t know that medicine could be like this.
In observing abortions and conversations surrounding sex and birth control, I watched women of all ages make careful decisions about their bodies, in conversation with their doctors about what would be the best choice for them and their lifestyles. I watched women make the type of decision that no one ever wants to make about terminating a pregnancy—older women and young teenagers, women alone and women with partners, each with her own story, her own reasons, and a heavy heart. And I watched them make that decision in an environment free of judgment and full of excellent care.
My second week there, I saw my first abortion procedure. I have worked for a surgeon so I’m used to procedures, and one of the residents gave me a really comprehensive explanation of what was about to happen and warned me that it could be bloody. Once the fellow, the resident, and I were in the room, however, my role changed from shadowing medical student to emotional support/hand-holder. It was difficult, it was unpleasant, it was bloody. The patient sobbed. I held her hand, I rubbed her shoulder. Abortion is not pretty, it is not pleasant, it is not easy. But it is absolutely necessary that women have access to it. And in that moment it became clear that I absolutely must know how to do this, that in these moments, I want women to be in rooms like this one where they are safe and supported.
Spending time in this clinic proved that a type of medicine I had only imagined is actually possible, and if it’s happening in the Bronx I have to believe that it could be a reality elsewhere. I don’t know how I got so lucky, but I sure am overwhelmed with gratitude for the opportunity to witness such incredible doctoring. I knew that it would be a learning experience but I didn’t expect it to have such an impact on my future and on my career. I came away from my RHE absolutely committed to becoming an abortion provider and with a new sense of focus, along with some really incredible role models and mentors.
By Felipe on June 21st, 2018. Posted under: 2018
For 25 years, Medical Students for Choice (MSFC) members in medical schools around the country and the world have fought for the education they will need to provide a full range of family planning care for their future patients. For most of our members, learning about all forms of contraception and abortion is hard, and in some places, impossible…despite the fact that most of their future patients will rely on family planning throughout their childbearing years.
In May, the Trump administration proposed a new rule for family planning clinics receiving federal funds appropriated by Congress to care for low income people. This rule would overturn more than 40 years of requiring that the care provided in these clinics provide patients with information on all their options when facing an unintended pregnancy. This new rule is commonly called “the domestic gag rule.” If the “gag rule” goes into effect, health care workers in clinics funded by the federal family planning program will be prohibited from talking with patients about abortion, may not provide information to patients about where to go for an abortion, and may not provide abortion services to those patients even if it is in a separate clinic with separate funding.
MSFC has worked for 25 years to incorporate the full range of family planning care – including abortion – into medical education and training. Through this work, we are gradually eliminating the stigma against abortion that exists within medicine. We believe that no one should have to face additional barriers when seeking this common, safe, and simple medical procedure. The Trump administration’s “gag rule” formalizes abortion stigma, makes abortion less safe by creating barriers to access, and harms the health and well-being of those in our communities who need our support most.
We all know that the true target of these new rules is Planned Parenthood. Despite the fact that Planned Parenthood has played an essential role in providing access to critical family planning care in over 900 communities throughout the US for over 100 years, the organization has become a focal point of anger on the part of Republicans who oppose all that Planned Parenthood stands for – equity, access, and respect for all those in need of family planning. By attacking one organization through this rule, the Trump administration will hurt all families in need and ensure a lower standard of health care for those who rely on federal funding to support their access to family planning care.
MSFC is dedicated to ensuring that medical professionals have the education they need to provide the very best family planning care available in our country – to anyone in need of that care. The “gag rule” will make that impossible. Please stand with us and post your comments in opposition to these rules at https://www.regulations.gov/comment?D=HHS-OS-2018-0008-0001.
By Felipe on May 17th, 2018. Posted under: 2018
In 1983, Ireland held a referendum on what became the 8th amendment to their constitution. This vote determined that the fetus’s right to life was equal to that of the mother. 35 years have passed in Ireland since the 8th amendment formally outlawed abortion in the Irish constitution, but since then there has been a perceived shift of the younger generation becoming more progressive. On May 25th, Ireland will hold another referendum, this time to repeal the 8th amendment and make abortion legal in Ireland.

Our four Irish chapters have been educating medical students about reproductive health and rights for years but have never been able to provide abortions in their own country. With the possibility of the 8th amendment being repealed, these Irish students may become the first generation of abortion providers in their country. I spoke with some of our Irish chapters to understand why this referendum has come about, their personal beliefs on abortion, and their hopes for the future of abortion provision in Ireland.
The Setting: Recent History and Religion
Since the referendum in 1983, Ireland has voted several times to establish guidelines about abortion. In 1992, the 13th amendment stated that the government could not limit travel of an individual abroad to have an abortion. Similarly, the 14th amendment made it legal for health professionals to provide information about abortions abroad. According to the UK Department of Health, nearly 170,000 Irish women travelled to the UK to have an abortion since 1980. In 2013, legislation was passed to allow abortions in cases of threat to the life of the mother (including suicide), but, according to Matthew Parsons, a student at the School of Medicine Trinity College Dublin, “due to ambiguity in the law… healthcare professionals are hesitant to attempt abortion even when medically indicated.” An MSFC Student Leader at the University of Limerick, Róisín Gryson, pointed out that all these amendments have, “resulted in people in Ireland not getting full access to medical care whilst pregnant and [have] resulted in tragic deaths”.
Impacting every aspect of this issue is the Catholic Church. Ireland is a predominantly Catholic nation with a historic relationship with the Church, which strongly opposes abortion. Catholicism has long been an important part of Irish society and has influenced political matters even before Ireland became a country. Our Irish members noted that the Catholic Church was involved in the introduction of the referendum in 1983, and the result of the referendum was influenced by religion’s role in the lives of Irish citizens. Though many people are both religious and pro-choice like those in the organization Catholics for Choice, religion played a large role in the successful campaign to restrict abortion.
Because the 8th amendment was passed 35 years ago, no one under the age of 55 voted in that referendum. Many note that the younger generation in Ireland is more progressive on social issues, as evidenced by contraception and gay marriage becoming legal. But even with a perceived change in attitudes, abortion stigma remains a very strong force. To fight this, Róisín noted that “as the referendum draws closer, brave women are coming forward and telling their personal stories”. In Her Shoes is a Facebook page that shares women’s abortion stories to bust myths surrounding abortion.
Today’s Activists

Róisín said her passion for abortion access stems from her “fundamental thought that all people deserve patient autonomy and the right to make their own choices about their healthcare.” Our Irish chapters spread their passion and fight stigma everyday by putting on events educating their peers about abortion, reproductive health, and rights.
This April, Trinity College Dublin’s MSFC chapter hosted an event called ‘Chats for Choice’, where representatives from Doctors for Choice, Lawyers for Choice, Psychologists for Choice, among others, discussed the referendum and the issues surrounding the vote, including the spread of misinformation. Together, all the representatives of these groups signed a statement on repealing the 8th amendment and promised to, “combat the rise and spread of sensationalism, with evidence based information surrounding reproductive healthcare”.
At the University of Limerick, Róisín and other MSFC members at her medical school have been encouraging students to register to vote in time to participate in the referendum, and Róisín herself has gotten canvassing training to advocate for the Repeal the 8th movement. As Katherine Hughes from Trinity College Dublin put it, “doctors and med students have a role and responsibility to engage and inform the general public on the health implications of the current law.”
These medical students are committed to abortion legalization and access, which makes me optimistic about the result of the referendum on May 25th. Matthew hopes that, “abortion will be allowed in Ireland without the need for an abortion panel of physicians.” Likewise, Róisín wishes, “that Ireland in the future will be a place where everyone has control over their reproductive rights and that doctors can provide for their patients according to their wishes and best interests”.
If the 8th amendment in Ireland is repealed and abortion becomes legal, Medical Students for Choice members will be the first generation of abortion providers in their country. Róisín reflected, “Prior to medical school I had always thought I would not be comfortable providing abortions. However, I have come to realise that it will be my duty as a medical professional to provide the best care I can for my future patients.” Should Ireland legalize abortion, our members will make sure it becomes accessible and a reality.
By Felipe on May 08th, 2018. Posted under: 2018
You may be looking at the title and thinking, “yeah, duh.” But there are two things you should remember. The first is that good medicine relies on scientific evidence. Think back to the kerfuffle over flossing in 2016 (a more innocent time, to be sure). The AP reported that this mundane, common-sense dental hygiene task did not have many long-term studies to back it up. People were up in arms over it! Interestingly, in a rebuttal article, a dentist wrote, “At the end of the day, flossing is your call. Patient autonomy is essential to health care.” Perhaps we could all apply the same sentiment to the rest of a woman’s body.
The second thing to remember is that most people have a significant knowledge gap when it comes to abortion. Many people don’t know that abortion is a common procedure, one that a quarter of American women will have by the time they are 45. They don’t know all the hoops women and doctors have to jump through to get it or provide it, respectively. Perhaps most importantly, people don’t know how incredibly safe abortion is. Fear and emotion often rule a conversation about abortion instead of facts and science.
Science is the foundation of all medicine, and abortion is a part of medicine. Peer-reviewed reports that back up the safety of it put a significant damper on the anti-choice argument that women need to be protected from this procedure. This research refutes the many laws being introduced that allege abortion is unsafe and therefore must be regulated to extinction. We trust science, and we trust women.
The Study
In March, the National Academies of Sciences, Engineering and Medicine (NASEM) released a new report which concludes that abortion in all forms is safe and effective. This evidence-based, nonpartisan, scientific research review, which was developed by an independent panel of 13 experts in the field, is the first comprehensive look at abortion safety, access and care conducted in the last 40 years.
Here are the key takeaways:
Abortion Is Safe
The NASEM report concludes that all forms of abortion – medication, aspiration, dilation and evacuation (D&E) and induction – have very low rates of complications, with some as low as a fraction of one percent of all patients. Further, the report notes that abortion has no impact on a woman’s future fertility, breast cancer risk or likelihood to experience mental health disorders.
The research also finds that in most cases, abortion care doesn’t require special equipment or emergency arrangements. Moreover, the research explains that a trained physician, physician assistant, certified nurse-midwife and nurse practitioner has the skills and experience to perform most procedures.
Medically Unnecessary Regulations Impact Quality of Care
While politicians across the country seek to limit access to abortion care, NASEM’s research finds that these regulations are not only medically unnecessary, but they also negatively impact women’s quality of care. To reach this conclusion the researchers reviewed abortion against the Institute of Medicine’s (IOM) attributes of health care quality and found that medically unnecessary regulations impact five of the six quality attributes: effectiveness, patient-centeredness, timeliness, efficiency and equity of care (safety was the only attribute not impacted by regulations). The report defines medically unnecessary regulations as “[limiting] the number of available providers, [misinforming] women of risks of the procedures they are considering, [overruling] women’s and clinicians’ medical decision making or [requiring] medically unnecessary services and delays in care.”
Specifically, the report invalidates medically unnecessary regulations including requiring a licensed physician perform abortion, requiring informed consent to include inaccurate information on long-term effects, mandating medication abortion only be taken in the presence of a clinician and requiring clinics to have standards equal to surgical centers or a certain distance to a hospital.
To learn more about the report, visit www.abortionissafe.com.
By Felipe on April 30th, 2018. Posted under: 2018
By RWAMIYE J. Pavel, University of Gitwe
This February, over 250 students in multiple medical fields all over Rwanda (and abroad as well) gathered for a joint 3-day conference at the University of Gitwe. This conference, organized by our MSFC chapter in partnership with numerous other organizations, was entitled “The Role of the Youth in Addressing the High Number of Unsafe Abortions and their Complications.” We brought together medical, nursing, and pharmacy students; general practitioners, and other healthcare professionals; and several NGOs from Rwanda and abroad, including the United Nations Population Fund, Health Development Initiative, the Rwanda Biomedical Council, and African Youth and Adolescents Network (AfriYAN). We were also very happy to welcome our fellow MSFC Chapter at Makerere University in Uganda, who honored us with their presence and made successful contributions to the conference.

Pavel, the author, is on the left.
Rwanda is still a conservative society, although in larger cities the mentality is evolving. Abortion is only legal in Rwanda in cases of rape, incest, forced marriage and fetal impairment. Additionally, Gitwe is a very religious community, and abortion is strongly stigmatized although cases of induced abortions have been reported at the Gitwe Hospital. Even a pregnant woman who fits all the legal criteria for receiving an abortion (i.e is pregnant by rape or incest or who has a risky pregnancy) has to go through a long process which involves consulting at least two practitioners.
That serious matter happens to be our next move on the long journey of completely legalizing abortion. The conference attendees were committed to making significant change in simplifying the difficult process of obtaining a legal abortion, and we also discussed the necessity of reducing restrictions on abortion overall. Our speakers emphasized the numerous cases of women in prison because of abortion cases, and participants were shown testimony from girls who are serving time because they have been convicted of abortion.
The University of Makerere MSFC Chapter presented in a plenary session on abortion laws and access in Uganda, where laws are also very restrictive. The only difference between the two country is that in Uganda, they have many illegal suppliers that provide the population with abortion pills. Critical care is also provided easily in case of a self-induced abortion when the patient goes to the hospital.

Being in a religious community poses challenges to our work. As our university is a Seventh-Day Adventist school, our MSFC chapter is not recognized by the administration. Therefore, we hosted this event in partnership with the University of Gitwe Medical Student Association (UGMSA) and were able to host the event in their name. At the end of the conference, most of the participants were convinced that abortion legislation must be improved and supported the idea of reducing barriers to accessing legal abortions, while still considering Rwandan traditions. Through this conference, we reached a large number of students who will return to their communities and advocate for safe abortion throughout their careers. Many were interested in becoming MSFC members.
I think my education is behind all my activism. I was raised by a mother who could not tolerate gender inequality. My mother was a history teacher, and since we were very young, she taught us to respect every person regardless of their race, ethnicity and opinion. Facing gender discrimination in her career as a teacher, she quit and took evening courses on gender equality. After graduating, she became a women’s rights activist, and she now teaches other women in the countryside how to become independent.
This is what inspires me and makes me want to do something for all those women that are still under the oppression of our patriarchal society. The injustice toward women in our traditional society must stop, and we shall give women what is due to them since the beginning: the right to make choices about their body as they want! The time has come where all individuals shall be treated equally, and each and every person on this very Earth shall be free.
By Felipe on March 23rd, 2018. Posted under: 2018
Hello from Buffalo, NY! We are second year medical students at the University at Buffalo Jacobs School of Medicine and co-presidents of the MSFC Buffalo chapter. One of the unique activities we coordinate as part of our chapter is contraceptive counseling at the Lighthouse Free Clinic.
Lighthouse Free Clinic is a medical student-run organization that partners with community physicians to provide free healthcare to uninsured and underserved patients in Buffalo. The clinic provides a range of primary care services including contraceptive counseling by our MSFC volunteers. Patients can indicate on their intake forms whether they are interested in seeing a contraceptive counselor during their visit or if they are referred from the clinic’s STD testing services.
The MSFC contraceptive counseling program began two years ago as a result of conversations with the student managers of the Lighthouse Free Clinic. The managers reached out to MSFC about the need for birth control information and education among the patient population, and so MSFC partnered with some of Buffalo’s OB/GYN residents to establish trainings for medical students interested in volunteering at the Lighthouse Clinic. Bryna Torre, currently a third year medical student and the founder of the University at Buffalo chapter of MSFC, spearheaded the program’s development.
Bryna grew interested in birth control education while doing research into the impact of contraceptive counseling. “I myself was never counseled on birth control by my doctors, and I’ve spoken with one too many women who felt their only option was the birth control pill despite there being much more effective and convenient methods available. I believed that the best way to overcome this lack in knowledge amongst patients was to go straight to the medical school and provide opportunities for future physicians to become educated on birth control. Our hope was that medical students would carry these skills with them for the benefit of their future patients as they enter their clerkships, and ultimately their careers.”
Following Bryna’s direction, our goal as MSFC volunteers is both to educate our peers about reproductive health and birth control, and also to share this information with patients at the clinic. We hope that our services inform patients about birth control options and empower them to make safe, personalized decisions about the care that is best for them.
Contraceptive counselors at the clinic are all medical students who have undergone a training session, which is organized and run by our MSFC chapter, using materials assembled by previous student leaders. In training, we discuss the different birth control options available, the methods by which these options work to prevent pregnancy, side effects, and the contraindications. We also teach our volunteers how to conduct the counseling interview, how to get a prescription for the patient at the clinic, and where to refer them in the event that they choose a method we cannot provide. At the Lighthouse Free Clinic, we offer free condoms, and our physician volunteers can prescribe the pill, the patch, or the ring. We typically refer out to Planned Parenthood and other local clinics for any other form of contraceptives (including IUD placement).
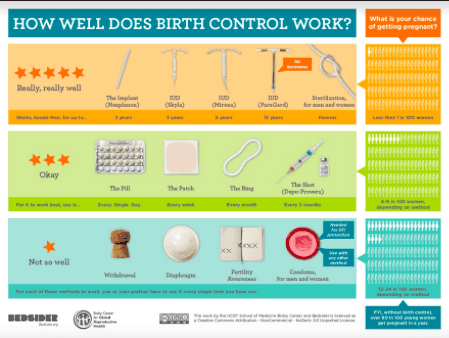
We start out with a questionnaire to get to know the patient and their needs better, including what forms of contraceptives they have used in the past and why they liked it or not, as well as if there is any family or past medical history that would indicate high risk for hormonal methods. Then we run through a visual diagram of different forms of contraceptives, starting from the most effective (IUDs, implants), the next effective (the pill, the patch, the ring, the shot), and least effective (pull out method, fertility awareness). We always end by stressing that though we recommend using the most effective forms, condoms are the only way to prevent STD transmission. We like to use Bedsider.org’s diagram to guide our discussion and to hand to the patient for reference.
We are grateful to have this opportunity to have a positive impact on the local community, especially those who are medically underserved, while at the same time practicing our skills and educating our peers about contraceptives. Please feel free to email msfcbuffalo@gmail.com if there are any specific questions you have for us regarding our contraceptive counseling program!
By Felipe on March 09th, 2018. Posted under: 2018
When people hear “Alabama,” obesity, poverty, extremist religious views, Roy Moore, and STI’s may come to mind. Not exactly positive things. While my home state doesn’t necessarily represent equality, choice, or social justice, I have been lucky enough to be part of a class of medical students who (for the most part) do. My peers and I are not only advocating for fair and equal treatment of our future patients, including transgender patients, but also ensuring that those patients have access to appropriate care and control of their own health.
I attend the University of Alabama School of Medicine, which provides no formal training on treating LGBTQ+ patients, so students must seek out information provided by groups like MSFC and MedPride. MedPride is an organization of medical students, residents, allies, and physicians who inform students on LGBTQ+ individuals and their health, work to reduce stigma, and advocate for the rights of LGBTQ+ individuals. Our MSFC and MedPride chapters, along with a few other groups, recently held an event to fill these gaps in the curriculum and educate our peers on treating transgender patients. I represent MedPride as well as MSFC, and we knew this event was important because transgender youth are a vulnerable population.
 Alabama is not a receptive or supportive place for transgender individuals, and many patients avoid healthcare because of the fear of how they may be treated. Like other sexually active people, transgender people are at risk for STIs and unplanned pregnancies, but a third have delayed seeking preventative sexual health care due to the likelihood of being discriminated or disrespected. Plus, in a nationwide survey, 50% of trans people reported having to educate their health care provider on how to provide appropriate trans care. Medical students must understand that everyone, no matter their gender identity, has the right to control their body and have quality health care, including their family planning needs. We wanted to provide our fellow students with an open, judgment-free space to have their questions answered, clarify misconceptions, and provide information that will aid in the treatment of transgender patients in the future.
Alabama is not a receptive or supportive place for transgender individuals, and many patients avoid healthcare because of the fear of how they may be treated. Like other sexually active people, transgender people are at risk for STIs and unplanned pregnancies, but a third have delayed seeking preventative sexual health care due to the likelihood of being discriminated or disrespected. Plus, in a nationwide survey, 50% of trans people reported having to educate their health care provider on how to provide appropriate trans care. Medical students must understand that everyone, no matter their gender identity, has the right to control their body and have quality health care, including their family planning needs. We wanted to provide our fellow students with an open, judgment-free space to have their questions answered, clarify misconceptions, and provide information that will aid in the treatment of transgender patients in the future.
Our event focused on transgender and gender-variant youth. We collaborated with Nuts About Peds (our pediatric interest group), Psychiatry Interest Group, and the Office of Diversity and Inclusion (ODI). The panel was mainly made up of pediatricians, one general, one endocrinologist, and one psychiatrist, two of whom work at the transgender youth clinic held in the area. The panel also included a representative from a local LGBTQ+ organization that provides healthcare and community, including youth outreach. Having pediatrics, psychiatry, MSFC, and ODI involved helped students realize that regardless of their field, they will have transgender patients. They owe it to their patients to be as informed as possible about their care. 70 people attended, which is a great turnout in such a conservative area. We discussed how to make transgender patients comfortable and emphasized specific health concerns of transgender youth such as gynecological care, education on contraception options, and potentially storing sperm/eggs for future use in youth before they begin transitioning. The panelists highlighted that each patient is different and that physicians must allow patients to take the lead in determining what kind of medical transition they seek (if any). Attendees were very engaged and expressed interest in doing an additional panel to discuss the topic further.
Our efforts to educate our peers has caught the attention of the school administration. As a result, our curriculum may soon change for the better. ODI staff are currently creating an LGBTQ+ elective course that will hopefully be available soon. I’m proud to be a part of movement bringing education on LGBTQ+ health care to a public medical school in one of the most conservative states in the nation.
I wanted to host this event because providing a safe, inclusive, accepting environment for patients is essential to me as a future pediatrician. When patients come to my office, I want them to know every person they encounter has their happiness in mind and is an ally and resource for them. Reproductive rights and trans rights are important because every patient has the right to make decisions about their own body. Regardless of what specialty physician they see, patients should have access to the information and resources that they need. Events such as this one play a role in ensuring that future healthcare providers create a supportive environment for their patients and treat them with the respect that they deserve.
By Felipe on February 22nd, 2018. Posted under: 2018
Parvaneh (“Pari”) Nouri, an MD/MPH candidate at Wright State University Boonshoft School of Medicine, has testified three times against anti-abortion bills in the Republican controlled Ohio state legislature, and she’s gearing up for a fourth – a D & E ban has been introduced. In a hostile state like Ohio, advocacy work can be discouraging, but Nouri doesn’t let that stop her. She believes these anti-abortion bills create a “resource drain” of future and current ob-gyns, thereby harming the entire medical field, in addition to the dangerous barriers they create for patients. As a medical student and student leader of Wright State’s Medical Students for Choice (MSFC) chapter, Nouri wants to make her voice heard.
In the last six months, Nouri has testified in the Ohio house and the senate against the Down syndrome abortion ban bill and again in the house against the fetal heartbeat bill. “Each time I testify, I try to frame my argument in regards to how these laws will impact medical education, how medical students will make choices on residency, and how this will impact where physicians practice due to legal restrictions on the reproductive care services they can provide.” Nouri is intent on speaking from her unique stake in these issues as a future family planning provider.
This sentiment was echoed by Noel León, a lawyer with the National Women’s Law Center, who states that ob-gyns and residents may determine where they practice based on the reproductive health training legally available in each state. States hostile to abortion access create obstacles for providers. In determining abortion related legislation, lawmakers often overlook the medical perspective completely. “Lawmakers often know little about abortion, what it looks like, and how it affects other kinds of health care,” says León, “It’s important for them to hear: if you restrict training and abortion services, you make it more difficult for physicians to work with pregnant patients generally.”

Despite the lack of medically informed decision-making and the efforts of pro-choice advocates like Nouri, anti-choice bills, like Ohio’s upcoming D & E ban, will continue to crop up. The Down syndrome bill, HB214, was signed into law by Gov. Kasich and will go into effect in March of 2018. In 2016, Gov. Kasich vetoed the heartbeat bill and simultaneously signed a 20-week ban, but the heartbeat bill is now moving through the state legislature once again. Nouri sees no other option than to continue to push back.
After being contacted by the Vice President of Government Affairs and Public Advocacy for Planned Parenthood Ohio, Nouri first testified against SB164/HB214, which bans abortions in cases of a prenatal Down syndrome diagnosis and criminalizes physicians who perform an abortion in these cases. “Planned Parenthood or NARAL will reach out before every reproductive health related bill that comes through the state congress and often provide an executive summary,” Nouri explained. “Planned Parenthood and NARAL reps have even offered to edit my testimony, and submit it on my behalf.” This support makes it feasible for a busy medical student to participate in advocacy, as local organizations provide information on the legislation, the legislative committee, and hearing dates.
Ultimately, patients are the victims of legislation that strips away access to reproductive health care, but the medical community can and should advocate on their behalf. León points out, “Patients sharing their own stories about abortion is incredibly powerful and important, but abortion stigma makes it hard for many patients to feel comfortable being public. Residents and physicians are able to speak to patient experiences in a way that can be hard for patients to do.” Although many medical students don’t yet have patient experiences to draw from, León thinks student voices still carry weight. “Testifying fortifies a student’s confidence to speak up in the future for the next abortion restriction proposed. Additionally, it is important for lawmakers to hear from the next generation of health care providers, whether they become abortion providers or not, saying ‘access to abortion is important and this bill is harmful’.” Medical students, residents, and physicians have the expertise to highlight the medical ramifications of anti-choice bills to lawmakers who are unaware of the collateral effects their legislation will have.
When testifying against the fetal heartbeat bill, Nouri concluded with an appeal for her future as a physician providing reproductive care. “Our healthcare system and government have the great potential of operating as a mutual partnership; one that facilitates positive patient outcomes and preserves our global leadership in the highest standard of care. As a physician, I want to serve my patients under that standard of care, regardless of which state I practice in.” For medical students planning on being providers in hostile states, advocacy skills will prove essential. Their careers, and the patients they serve, will depend on it.
If you are a medical student or resident and are interested in testifying before your state legislature, please read our guide and contact MSFC student organizers at students@msfc.org for additional help.