By Felipe on June 30th, 2015. Posted under: News and Views
A state court judge just temporarily blocked a new law that forces women to wait 24 hours or more and make at least two trips before accessing safe, legal abortion care. Medical Students for Choice is a plaintiff in a lawsuit filed by Center for Reproductive Rights and the American Civil Liberties Union against the State of Florida challenging this law. MSFC board members, students and alumni are all getting involved to make sure Florida women can access safe, legal abortion care unhindered by burdensome waiting periods.
Future doctors and pro-choice physicians should be able to give women the care they need, when they need it. If this medically-unjustifiable law goes into effect, physicians who provide abortions will be forced to deliver care that is not in the best interest of patients. See below for the press release about the suit, and to find out why this law needs to be defeated!

State Court Blocks Florida Law That Forces Mandatory Delay, Additional Visits for Women Seeking Safe, Legal Abortion
June 30, 2015—(PRESS RELEASE) A state court judge today blocked a recently passed Florida measure forcing a woman to wait at least 24 hours and make at least one additional trip before she is able to receive safe, legal abortion care. The law—which was slated to take effect on July 1, 2015 and will remain blocked while the case proceeds– fails to include any protections for a woman whose pregnancy threatens her health or a meaningful exception for survivors of rape, incest, or intimate partner violence.
“Women are fully capable of making thoughtful decisions about their lives, families, and health care, and this ruling will keep them from being second-guessed or delayed by politicians who presume to know better,” said Autumn Katz, staff attorney at the Center for Reproductive Rights. “We will continue to fight this demeaning law until the courts permanently strike it down and ensure no Florida woman is ever forced to wait for purely political reasons to get the health care she needs.”
The Center for Reproductive Rights, the American Civil Liberties Union, the ACLU of Florida, and Richard Johnson of Tallahassee challenged the unconstitutional measure earlier this month on behalf of Bread and Roses Women’s Health Center—a Gainesville reproductive health care provider—and Medical Students for Choice—an organization dedicated to making reproductive health care, including abortion, a part of standard medical education and residency training.
“This decision supports the right of all women patients to make the healthcare decisions they feel are most appropriate for them and enables their physicians to support their decisions,” said Lois Backus, Executive Director of Medical Students for Choice. “We are grateful for the court’s decision today.”
Waiting periods can create a variety of burdens on a woman who needs safe and legal abortion care—from stigmatizing women and abortion providers, to requiring additional trips to the clinic, which means additional travel time, transportation costs, child care, and time off work. Women of color, low-income women, rural women, and women in abusive relationships already face challenges when they seek health care services, and waiting periods only increase these barriers. Additionally, mandatory waiting periods can lead a woman to delay the abortion to later in pregnancy, which can increase the risks of the otherwise extremely safe procedure.
In a region devastated by similarly underhanded restrictions, Florida’s strong state constitutional protections have ensured the state serves as a safe haven for women from neighboring states seeking safe and legal abortion services. From clinic shutdown laws—which have closed clinics in Texas and threaten to shutter abortion providers in Louisiana, Oklahoma, Mississippi, and Alabama—to outright bans on abortion, women in the South often face innumerable hurdles when trying to exercise their constitutional right to safe and legal abortion services.
Harmful restrictions like these further underscore the need for the federal Women’s Health Protection Act (S. 217/HR. 448)—a bill that would prohibit states like Florida from imposing unconstitutional restrictions on reproductive health care providers that apply to no similar medical care, interfere with women’s personal decision making, and block access to safe and legal abortion services.
By Felipe on June 11th, 2015. Posted under: News and Views
Medical Students for Choice is a plaintiff in a lawsuit just filed by Center for Reproductive Rights and the American Civil Liberties Union against the State of Florida. The suit challenges a new law that forces women to wait 24 hours or more and make at least two trips before accessing safe, legal abortion care. MSFC board members, students and alumni are all getting involved to make sure Florida women can access safe, legal abortion care unhindered by burdensome waiting periods.
Future doctors and pro-choice physicians should be able to give women the care they need, when they need it. If this medically-unjustifiable law goes into effect, physicians who provide abortions will be forced to deliver care that is not in the best interest of patients. See below for the press release about the suit and to find out why this law needs to be defeated!

Center for Reproductive Rights and ACLU Challenge Unconstitutional Florida Law That Forces Mandatory Delay, Additional Visits for Women Seeking Safe, Legal Abortion
Measure is a blatant violation of Florida state constitution, lacks any medical justification
June 11, 2015—(PRESS RELEASE) The Center for Reproductive Rights, the American Civil Liberties Union, and the ACLU of Florida filed a lawsuit in state court today which seeks to block a recently passed Florida measure forcing a woman to wait at least 24 hours and make at least one additional trip before she is able to receive safe, legal abortion care. The law—slated to take effect on July 1, 2015—fails to include any protections for a woman whose pregnancy threatens her health or a meaningful exception for survivors of rape, incest, or intimate partner violence.
“Women are fully capable of making thoughtful decisions about their lives, health, and families without interference from politicians seeking to advance an agenda,” said Autumn Katz, staff attorney at the Center for Reproductive Rights. “We are confident this demeaning measure will be struck down as a blatant violation of the state’s strong constitutional protections for women’s rights.”
“It’s clear that the sole purpose of this law is to make it more difficult for a woman who has decided to have an abortion to get one, and to punish and discriminate against those who do,” said Renée Paradis, senior staff attorney for the ACLU. “Furthermore, it’s flat-out offensive. A woman who is seeking an abortion has already carefully considered her decision. She doesn’t need politicians to create additional hurdles because they disagree with her.”
“Physicians have an obligation to both provide and advocate for the care their patients need when facing an unintended pregnancy–and laws like Florida’s make that impossible,” said Lois Backus, Executive Director of Medical Students for Choice. “If allowed to go forward, this law will make it more difficult for women in Florida to obtain the quality healthcare they deserve for generations to come.”
Waiting periods can create a variety of burdens on a woman who needs safe and legal abortion care—from stigmatizing women and abortion providers, to requiring additional trips to the clinic, which means additional travel time, transportation costs, child care, and time off work. Women of color, low-income women, rural women, and women in abusive relationships already face challenges when they seek health care services, and waiting periods only increase these barriers. Additionally, mandatory waiting periods can lead a woman to delay the abortion to later in pregnancy, which can increase the risks of the otherwise extremely safe procedure.
In a region devastated by similarly underhanded restrictions, Florida’s strong state constitutional protections have ensured the state serves as a safe haven for women from neighboring states seeking safe and legal abortion services. From clinic shutdown laws—which have closed clinics in Texas and threaten to shutter abortion providers in Louisiana, Oklahoma, Mississippi, and Alabama—to outright bans on abortion, women in the South often face innumerable hurdles when trying to exercise their constitutional right to safe and legal abortion services.
The Center for Reproductive Rights, the American Civil Liberties Union, the ACLU of Florida, and Richard Johnson of Tallahassee filed today’s challenge in the Circuit Court of Leon County on behalf of Bread and Roses Women’s Health Center—a Gainesville reproductive health care provider—and Medical Students for Choice—an organization dedicated to making reproductive health care, including abortion, a part of standard medical education and residency training.
Harmful restrictions like these further underscore the need for the federal Women’s Health Protection Act (S. 217/HR. 448)—a bill that would prohibit states like Florida from imposing unconstitutional restrictions on reproductive health care providers that apply to no similar medical care, interfere with women’s personal decision making, and block access to safe and legal abortion services.
By Felipe on May 12th, 2015. Posted under: News and Views

By: Dr. Michelle Brown
As I reflect back on the 4 years of medical school that I just completed, MSFC has been an integral part of my experience here. The support that MSFC provided over the past 4 years for me personally and professionally has been incredible. One of the highlights of my involvement with MSFC was attending the Activist Leader’s Institute, a weekend-long event that brings together medical students from across the country to identify areas of potential change and to train students in discussing the need for abortion-related education with the both media and their medical school higher-ups (this content is now shared through the student organizing program). This experience empowered me to speak up when a recent bill severely threatened medical education in North Carolina.
The Dangers of House Bill 465
House Bill 465 was proposed by the NC House and would create a number of large abortion restrictions in our state. The bill included many provisions, including lengthening the waiting period before a woman could have an abortion from 24 to 72 hours, creating burdensome paperwork restrictions for providers who perform abortions, limiting the scope of who can perform abortions to OB/Gyns, and perhaps most alarmingly, a provision that would ban abortions from being performed at UNC and ECU hospitals, the hospitals affiliated with the two public medical schools in our state.
As I was reading about the law, I was very concerned about the implications on the education of my peers. This new law threatened to make education about abortion inaccessible for medical students and residents at UNC and ECU. Exposing medical students to abortion and training residents how to perform procedures is vital to ensuring North Carolina women have the comprehensive care the need and deserve.
Taking Action
Shortly after hearing about the law, a friend asked me if she could pass my name along to a colleague who worked at Planned Parenthood and was looking for residents and medical students who would be impacted by the law. My friend wasn’t involved in the medical field- she was a Philosophy student that I knew from playing in an orchestra. However, she knew that I would be a receptive audience member due to the fact that I was vocal about my involvement in MSFC in the past. It was a great reminder that everyone you meet can have connections to reproductive rights activism, and that simply engaging friends in conversation can lead to opportunities down the road.
The representatives from Planned Parenthood were organizing a rally on the UNC campus against HB 465, and asked if I would be willing to speak about the law and its impact on medical education. I wrote a five-minute speech that summarized the impact this bill would have on the training of future physicians, the pipeline of future providers, and the availability of this important procedure for the women of North Carolina.
Tips for Advocacy
I knew there would be representatives from the media at this rally, so I consulted one of my friends who has prior experience in PR work. He helped rehearse some common questions with me, and gave me some tips on how to look on camera. His most important recommendation was to have a few talking points that you could write on the back of an envelope, and stick to those points. No matter what question you’re asked, redirect your answer to emphasize a talking point.
We also practiced answering questions that would likely come up, such as “What brings you here to the rally today?” and “What impact will this bill have on medical education?” Rehearsing the answers to those questions out loud a few times was really helpful. It was especially useful to have feedback on my overall appearance on camera- comments like “don’t move your head around so much” helped highlight distractions to my message that I wasn’t even aware of.
At the rally, I was joined by a Family Planning physician from my university and a pediatrician from a neighboring state who spoke about her personal experience with abortion. Having those other speakers there helped me realize how important it was to speak out, and helped bolster my confidence. I was the last to speak.
From watching the prior two speakers, I knew that the acoustics were less than ideal. I projected my voice to be especially loud and made a conscious effort to slow my speech to be more understandable. (I had to speak up even more when an a capella group started singing right next to us towards the end of my speech- awkward). By focusing on projecting and speaking clearly, I had the most understandable and audible speech of the 3 given that day- despite the impromptu concert.
While at the event, I made it a point to network both before and after my speech. I spoke to all of the event organizers and many of the attendees. I also followed up via email with the organizers afterwards. The day after the event, a representative from NC Policy Watch- a web site that follows North Carolina politics- emailed Planned Parenthood and asked if they would write an opinion piece on HB 465. PP representatives then asked me if I could rewrite my speech to fit into an op-ed format, which I agreed to do (you can read it here). After it was published, I got a lot of great feedback from friends in the community. Getting the concerns about this bill in a written format was really important for gaining traction and provided a convenient way to link to a summary my point of view to share with others.
Making Change
I was one of many, many voices that spoke up at rallies and in writing about the impact that HB 465 would have on medical student and resident education. The issue even got national attention with a piece in ThinkProgress. As a result of the onslaught of attention, the portion of the bill that would ban abortions from being performed at UNC and ECU was withdrawn.
This is a great relief to many faculty, residents, and medical students at these institutions. However, even with the changes that were made, HB465 is still an onerous bill that would force women undergoing abortion to have a 72 hour waiting period and would require documentation to be submitted to the state on abortions after 18 weeks for “statistical purposes”. By eliminating the portions of the bill with the most scrutiny- the portion that would prevent physicians from being trained- the bill is now more likely to pass through the NC Senate and become law. As always, the fight will continue. And, as always, medical students, residents and physicians have a powerful voice to use in that fight.
Michelle Brown is a recent graduate of the University of North Carolina School of Medicine and past president of the UNC chapter of Medical Students for Choice. She will begin her residency in Obstetrics and Gynecology at the University of Chicago next month.
By Felipe on April 06th, 2015. Posted under: News and Views
By: Taylor Stanton
Since I only discovered MSFC after my first year of medical school, I thought I had already missed my chance at taking part in the Reproductive Health Externship (RHE). It was at the annual conference on family planning that two important things changed: a fellow student suggested doing the RHE during my fourth year as elective credit, and Dr. Chastine was the closing speaker for the conference. Suddenly it clicked that I wanted to do my RHE down in Wichita, KS at Dr. Tiller’s re-opened clinic. It would be the perfect intersection of my own conservative town in which there are zero providers and my family planning rotation at Einstein in New York City, where access isn’t necessarily a problem. The first thing I did upon returning to Illinois after the conference was email Dr. Chastine and the clinic’s director to set up a rotation for the following fall.
I didn’t realize until I was eight hours into the drive that I probably couldn’t have picked out Kansas on a map, let alone Wichita. I was nervous that the couple I was renting a room from for the month would turn out to be anti-choice religious zealots and kick me to the curb. I was worried that I wouldn’t have any friends. Of course, driving up to the clinic the first day, everything changed. The clinic had such a warm feel to it, from the front door’s guard who joked with me as he scanned my bag to the quotes from Dr. Tiller on the wall of the lobby. Naturally, the front staff was amazing. When the clinical staff began to show up, an older spiky haired nurse took me under her wing to teach me the ins and outs of the procedures and the clinic. I was amazed to see a Thank You letter on their fridge that my MSFC chapter had made and sent to them nearly two years prior. It was only after our tour that one of the other nurses informed me that my guide was one of the original authors for Our Bodies, Ourselves. I was surrounded by history and those dedicated to making further history.
In the clinic I assisted with pre- and post-procedure ultrasounds and observed both first and second trimester abortions. Having already completed a month of family planning at Einstein, the procedures themselves no longer shocked me. A new challenge for me was the constant presence of protestors in the driveway. Whether the patient was a mother of five unable to afford another child or a woman devastated by the fact her very wanted fetus was anencephalic, she had to pass by grotesque signs held by protestors that recorded the license plates of everyone who came into the clinic. Windows had to stay rolled up lest they throw propaganda into your car and small crosses dotted the lawn. I was determined not to give them the time of day. If our patients could drive past them to receive our services, then I could pass them daily to help provide.
The other major difference from my experience in New York was the lengths our patients had to go to in order to even reach the clinic. They drove in from all neighboring states, even as far as twenty hours one-way from Texas, with its rapidly dwindling access. They found friends to stay with overnight if they were having a two-day second trimester procedure. They came up with money that, honestly, I don’t think I would be able to easily produce. But of course, these were the women I had envisioned helping when I decided to become a provider, and they were the reason the doctors, nurses, and staff at my clinic went to great lengths themselves to ensure the clinic stayed open.
Since my externship experience, I have realized my view of what it means to be a Provider has changed. Before this experience, I imagined that a doctor would only provide abortions full time or not at all. However, it is not as clear-cut: being a provider or not. The three doctors at the clinic worked there in different capacities and from three different geographical locations. Only one lived in Kansas . They each brought unique expertise while overall providing abortion and contraceptive care. Having worked with each of them, I realized that I had far more options for how abortion might fit into my future practice.
Looking toward my own future as a physician, a pursuit born from the simple desire to provide abortions for women who cannot get them easily, I am realizing that I do not know exactly where in the world of Family Planning I am going to settle. What I do know after my externship, however, is that I am reinvigorated to finish my studies and get out into the wider world. Unfortunately, women will most likely still be driving for days to reach our clinics, but I want to be the doctor there at the end of her drive to take care of her.
To find out more about the Reproductive Health Externship, join MSFC’s Google Hangout Q&A session on April 10th .
By Felipe on March 09th, 2015. Posted under: News and Views
I’m not sure that many people grow up thinking, “When I grow up, I want to be an abortion provider,” but I do think that a lot of people can imagine wanting to be a doctor so they can help others. For me, there are very few opportunities in medicine where a provider can offer a very basic and simple service to a patient who is in a very difficult situation and literally give them their life back. For the most part, patients are so grateful and relieved. It also provides a powerful opportunity to connect, offer resources, and empower a patient by teaching her how she can manage her fertility after the abortion.
After college, I worked for several years at a Planned Parenthood. Although initially I took the job because I am pro-choice and care about access to good comprehensive health care, the patients that I met gave me a clear new directive in life. For the first time I understood on a far more sophisticated level what the consequences of poor access to health care were and what the circumstances are of many women who are seeking abortions. I answered a hotline and I spoke to women all around the country who were looking for abortion services, and I realized how difficult it was to get accurate information, to find the clinic or a doctor that would provide the service, and to actually get there and pay for the abortion.
Abortion can be the last line of defense for women who live in desperate circumstances. Protecting abortion access—or rather, the right to choose whether and when to become a parent, is to me one of the most important components of my work in social justice. I believe that empowering women and their partners to manage their fertility successfully leads to stronger, healthier, communities where young people and adults have more opportunity to pursue their goals, and better circumstances if they decide to welcome children into their lives.
During medical school, I did research in contraception and became very involved in Medical Students for Choice, both in my local chapter and on the National Board. I attended a lot of reproductive health conferences and used every opportunity I could to network with abortion providers and other people who were interested in family planning. I did a Reproductive Health Externship in my fourth year to get more experience as well. In residency, worked with some of the mentors I had identified as a medical student and was able to set up almost all of my elective time for abortion and family planning training. Because of the relationships I had built over the years, a number of wonderful physician educators took me under their wings and I was able to train up to competency. After graduating from residency, I was very fortunate to get a job in a place that continued to support my education and training as well.
I am a family doctor, so my daily practice is a primary care clinic, where I see patients from all walks of life for all sorts of problems and preventive medicine services. If one of my primary care patients needs a medication abortion, I provide that service in my regular clinic. Once or twice a month, I also drive to another clinic about 60 miles away and provide surgical abortion services.
Without MSFC, I’m not sure if I would have been able to fulfill my dream of becoming an abortion provider. My medical school and residency curricula failed to educate me adequately about family planning and abortion care, so I had to seek out that education elsewhere. MSFC provided me with that knowledge–through lectures, conferences, externships, and most importantly, a community of great people who were always there for me. My work with MSFC laid the groundwork for getting involved in political advocacy, which is something that is very important to me now.
We, need to educate ourselves about the realities of poor abortion access, both so we can work to ensure that abortion will always be legal in the US and so we can advocate for our sisters in areas of the world where limited access represents a human rights emergency.
From a policy perspective, the past couple years have been devastating for abortion access in America. The sheer number and reach of TRAP laws that have been introduced and passed across the country have done more to erode access than at any other point in my lifetime. I am worried that the average person does not understand that there is a tremendously powerful political machine working in overdrive to create seemingly innocuous legislation that is in fact making abortion impossible for the most vulnerable women. This trend will only continue without a massive, coordinated, counter-movement.
Every time I meet a bright, excited, idealistic medical student or resident, I breathe a sigh of relief that the world is ok after all. I know many talented students and residents that understand the importance of abortion access and are committed to dedicating their careers to making a difference. When I look at how much Medical Students for Choice has grown over the years, and I see that there are now chapters in some of the most anti-choice places in the country and even the international community, I feel so proud of those students. They are working the movement, they are forcing change, and they are very, very brave.
As the saying goes, “if not you, then who?”

By Felipe on February 19th, 2015. Posted under: News and Views

Despite being part of the United Kingdom, abortion is treated differently in Northern Ireland. While abortion has been declared legal in Northern Ireland on certain health-based grounds, the guidelines for health professionals remain unclear. Though increasingly a topic of debate, many in Northern Ireland believe abortion to be completely illegal, and the countless barriers restrict abortion access only to women who can afford to travel to England to seek abortion care. Despite paying into the United Kingdom’s National Health Service, Northern Irish women who seek abortion care in other parts of the UK must pay out of pocket unlike all other UK citizens.
In a society in which abortion is highly stigmatized and restricted, the members of the Queen’s University Belfast chapter of MSFC have dedicated themselves to challenging their peers to improve their reproductive health education and to fight to improve the health care options for their future patients.
They held their very first event in December, a panel discussion on “International Women’s Health: Why Women Die” featuring expert panelists on medicine, human rights, and the history of abortion in Northern Ireland. As Kyle, a Queen’s University Belfast Student Leader, told me, “Our first event went really well, and had almost a hundred attendees. We got some great feedback and a couple of publications covered the event.” He continued, “From the event we developed both a mailing and members list – there are 25 people signed up to be members and around 90 on the mailing list.”
Following the overwhelming success of their first event, they held a hands on workshop on obstetrics emergencies just two weeks later which included a station on contraceptives and IUDs. Interest in that event was so high that they are already working on another contraception workshop at the end of February.
Hannah, another Student Leader at Queen’s University Belfast related, “It has been really exciting to be able to organize so many events, even more so that attendance has been so high! We are planning on running a few events this semester, including one entitled ‘Abortion: A Clinical Guide’ where we hope to explain abortion from a clinical perspective. We’ve received feedback from students that they would like to attend such an event, given that it’s not currently available on the QUB curriculum.”
We at MSFC HQ are so impressed with their work and we hope you will find it inspiring as well. Even in places that are extremely hostile to choice, medical students can and do successfully organize to promote education about family planning and reproductive choice!
By Felipe on January 28th, 2015. Posted under: News and Views
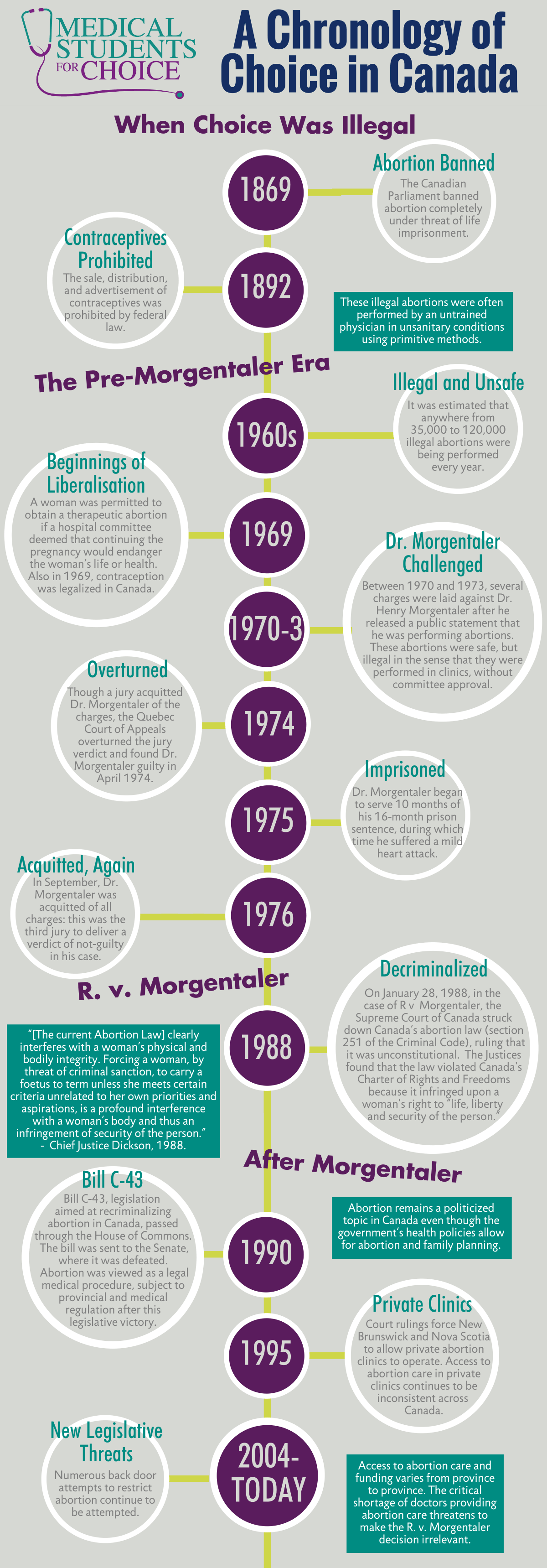
Over the years, the landscape of abortion access in Canada has changed dramatically thanks to hardworking activists and brave providers. However, even though government policies allow abortion in Canada, the topic is still highly contested. Recent restrictions on providers and a lack of training for physicians mean that in many places women still struggle to access abortion services. Here is how the ability to choose has changed over time in Canada:
By Felipe on January 21st, 2015. Posted under: News and Views
42 years since the Roe v. Wade decision guaranteed a woman’s right to terminate a pregnancy, we are still fighting for abortion access for all. Despite these barriers, medical students in the United States and around the world are advocating for greater access to reproductive healthcare, seeking out training, and stepping up to become the next generation of abortion providers.
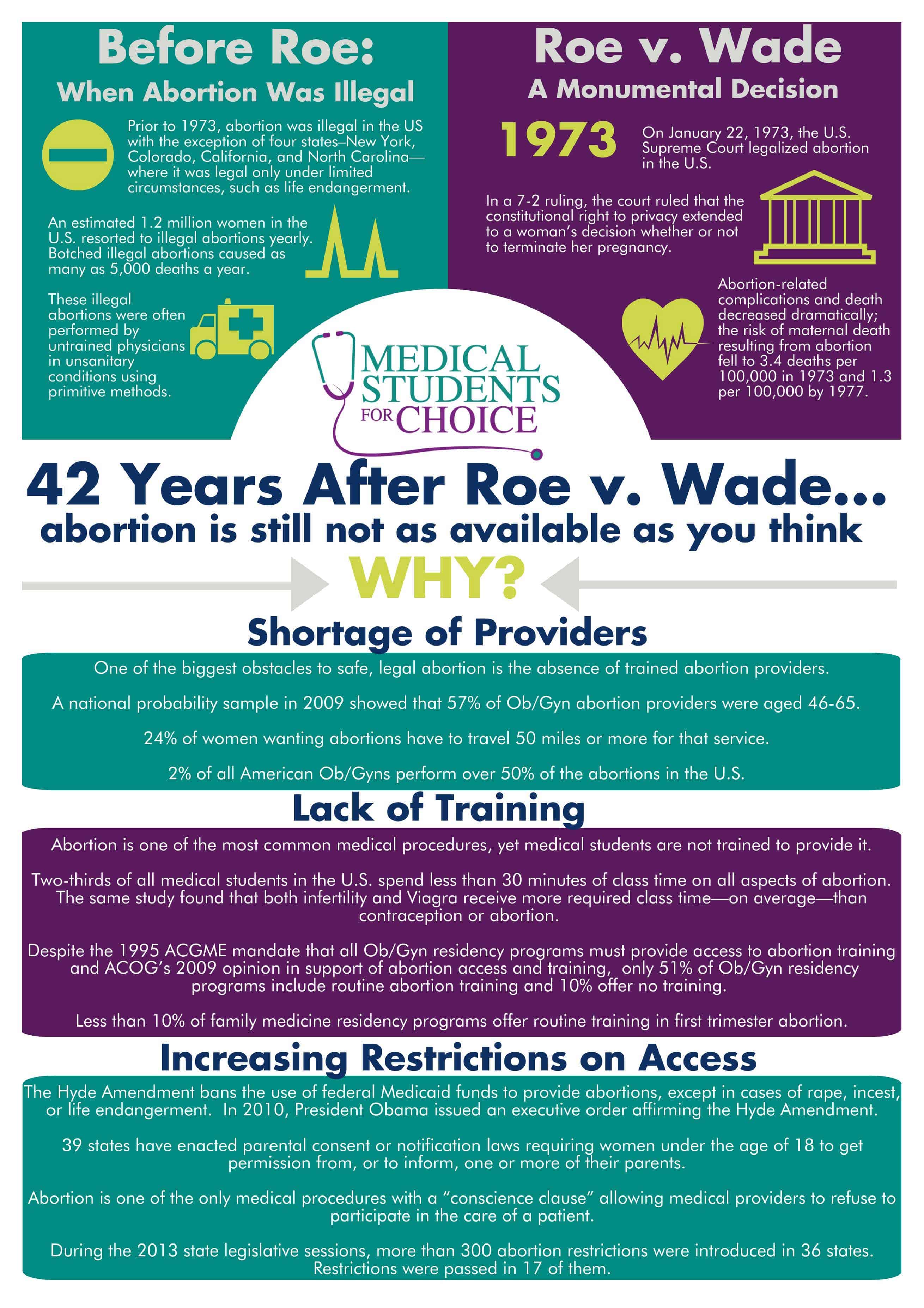
Downlaod pdf: 42 Years After Roe v Wade Fact Sheet
By Felipe on October 31st, 2014. Posted under: News and Views
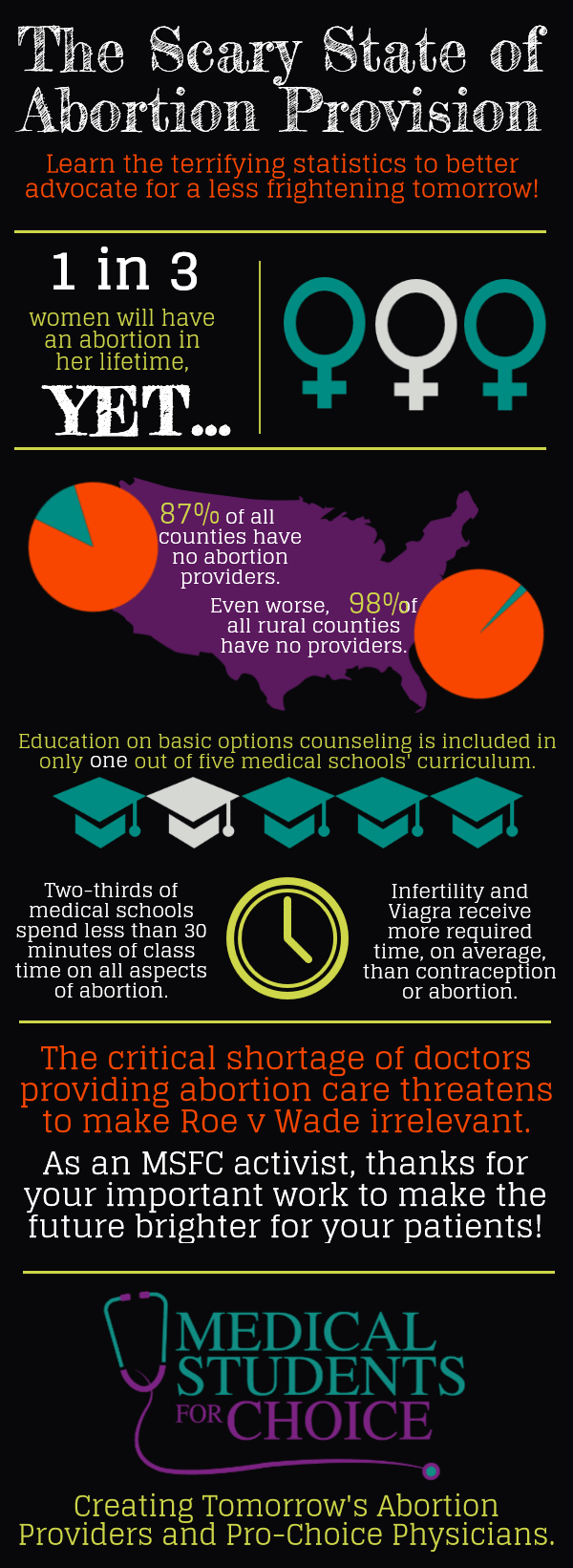
The critical shortage of abortion providers threatens the state of women’s health access.
By Felipe on October 20th, 2014. Posted under: News and Views

Despite running on no more than thirty minutes of sleep, my mind wouldn’t stop buzzing. Walking through Philadelphia International Airport, en route to MSFC’s Abortion Training Institute, I was curious about what the conference would entail—what skills I would learn, what experiences and opinions I would be exposed to.
For the most part I was excited. As part of a largely pro-choice undergraduate and medical community, I’ve been privileged with many opportunities to learn about abortion care and to engage in many conversations around reproductive justice. Each of these interactions, whether with classmates, providers or activists, has furthered and complicated my understanding of abortion care. I sought out the Abortion Training Institute because I wanted to keep learning: to keep having these conversations with diverse groups of people and to keep challenging my own assumptions about choice.
Challenging Assumptions
Our first workshop did not disappoint. Called the “Values Clarification Session,” it was an assumption-challenging power hour where we explored our biases and comfort levels with various aspects of abortion care. People engaged in debate over the meaning of viability and definitions of person-hood. When our facilitator brought up the issue of incarcerating pregnant women who refused treatment for drug addiction, I found myself confronting my own norms about pregnancy, childcare, and bodily autonomy. Who gets to decide what is best for a pregnancy? When do we take that control away from pregnant women? Seeing future physicians discuss their boundaries, in such an open environment, I realized how important values are in abortion care.
In the world of medicine, especially in reproductive healthcare, we’re often told about the importance of providing “non-judgmental, non-biased” care. What this session made very clear, however, is that bias and judgment are all unavoidable parts of clinical abortion and reproductive care. Healthcare providers are human, and will bring very human values to their work. As a future clinician, I’ll inevitably run across scenarios in my practice that will trigger me emotionally, or lead me to pass judgment on a patient based on my beliefs. But having biases doesn’t mean I’ll be compromising people’s care. Instead, by owning my assumptions and my values, rather than pretending that they don’t exist, I can be better prepared for these triggers when they come up. And more importantly, I can work past them to focus on providing the best care for the person in front of me.
Bringing Change
Reflecting on the Institute now there’s still much of the experience that stays with me. One physician mentioned during the provider panel that MSFC was the reason she stayed in medical school — a sentiment that greatly resonates with me. For much of my medical training thus far, I’ve felt bogged down by details of biochemical pathways and pharmokinetics, feeling removed from patient care. Since becoming a part of the MSFC community, I’ve begun to reconnect with why I wanted to become a doctor in the first place — to deliver care and bring change. As an abortion provider, I will not only be able to provide one of the most common yet most inaccessible medical procedures, but also provide knowledge, safety, comfort, affirmation, and reassurance.
MSFC’s Abortion Training Institute reminded me that without the work of fearless providers, there would be no choice.But let’s not forgot that a woman’s access to providers is only one part of her ability to choose. In a culture where women are shamed for their sexuality and denied access to affordable family planning, there is no choice. In a system where only wealthy women can access care, there is no choice. In a society where one out of six women experiences sexual assault, there is no choice. In a country that mass incarcerates women of color, sterilizes them without their consent, and denies them access to basic reproductive healthcare, there is no choice.
Even as a future provider, I know I won’t even begin to tackle most of these issues. But I’m grateful to MSFC for giving me a head start—for giving me both the clinical skills and the amazing network of providers, activists, and counselors tirelessly working for women and for choice. I hope to join them one day. Until then, I’ll be sure to keep learning, keep reflecting, and keep challenging.
 By: Gopika Krishna
By: Gopika Krishna